About 10 years ago I was building a practice in Edgewood. It was my first time really paying attention to the demographics of who I was treating and what trends I might be seeing in referrals. I recall one of the twenty-something Rehab Aides remarking, "so pretty much I should assume that when I'm 52 I'll have a shoulder problem"? (Ouch, I thought then...and again right now at 54. But, it was true. At that time I had a high volume of women in their 50's with shoulder pain. The trend, it turned out was that most were new to yoga, which was then in a really popular phase here in Pittsburgh. A sudden uptick in the volume of weight bearing through their shoulders, elbows and wrists, combined with shoulder blade and postural weaknesses made for this phenomenon. We don't spend much time on our hands so when we suddenly add even as little as 20 minutes a week of upper extremity weight bearing to our workout routines and something might give, especially if form is lacking. The relevance of age was simply that, beginning in our 40s and 50s our tendon tolerance changes. The aqueous base dehydrates a bit, the resilience is decreased, the preexistence of defects absorbed over years reaches a tipping point and pain occurs and now lingers unlike when we were younger. For those shoulder patients exercises, awareness, time training with better instructors and added strengthening for their core muscles helped immensely. There's another trend I am now seeing and that is men and women in their early 70s with outer hip pain. In the 1990s most of these folks would receive cortisone injections to the pointed part of the lateral hip and for some that would offer immediate relief and therefore the end of their desire to address the root cause of the pain. More current best practice suggests that the injection in to the trochanteric bursa may be more risk than benefit and not the best first line of treatment. So fortunately for me...here come those patients. But what is happening? Again an increase in weight bearing activity (walking usually, some runners) and a magnification of underlying weaknesses as well as age related tissue intolerance is most often the cause. Again this is a fixable condition with proper exercise and stretching. The multiple muscles making up the lumbopelvic region must work synchronously front to back and right to left side. The goal of the buttocks muscles is primarily to stabilize the hemi pelvis on the weight bearing leg so that the opposite, non weight-bearing limb, can swing through space and advance the foot for walking or running. If there is joint pain from any number of reasons in the weight-bearing hip it will hurt instantaneously (or longer) to contract all of the muscles properly when advancing the opposite leg. The person might try to consciously or unconsciously reduce that pain by leaning away from the pain, by failing to fully contract the muscles, by substituting with back or leg muscles, or by shortening their stride. If there is ineffectiveness from over tight muscles or simply under strong muscles the increased walking or running demands may accentuate these asymmetries. In a generation that fully embraced aerobic health when Jim Fixx first started running these Baby Boomers may walk through this pain and inflammation at the bursa causing it to no longer function properly and ache at night, and advance to nicks and tears in the gluteal tendons around the hip joint. Gluteus medius tendinopathy is a term likely to increase in our lexicon in the same way people talk about rotator cuff injuries and achilles pain. (Fabulous video link courtesy of my excellent home exercise platform Medbridge). Tissue intolerance and tendon breakdown in the rotator cuff muscles of the hip are as likely as in the shoulder. Fortunately this too can be addressed in physical therapy. And, while it may require a modification of your current walk/run program, open mindedness to cross training for different hip muscles stresses, footwear changes and with patience this too can pass! Let me know if this is something you can relate to and what has worked for you. Be good! 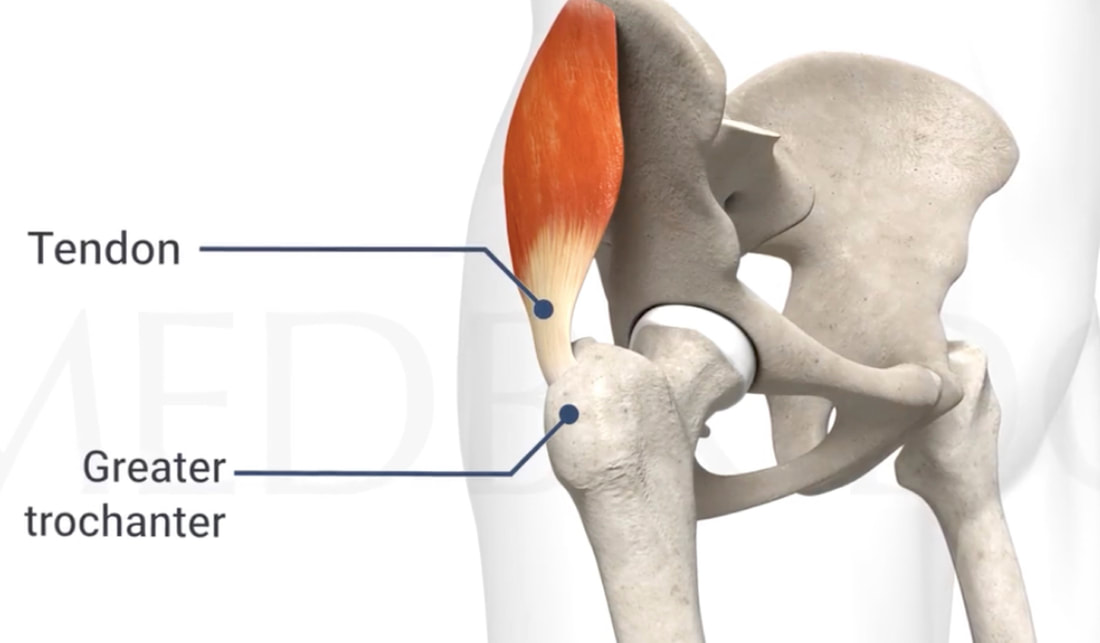 Comments are closed.
|
Author:
|


Perspectives for Patients:
 RSS Feed
RSS Feed
Proudly powered by Weebly