 I’m a little fascinated by the design of the microscopic coronavirus and have looked at tons of images of it. One of the more beautiful images is on a preceding post courtesy of the American Academy of Orthopaedic Surgeons. Admiring the virus, however is a bit like the fascinating yet psychopathic character Villanelle on the BBC show Killing Eve. The crown of proteins that are so cool to look at turn out to be exactly the destructive pieces that destroy critical cells in the deepest portion of the lung and cause a cascade that can kill. What I know so far is mostly from reading and listening to webinars by the Cardiopulmonary Section of the American Physical Therapy Association, the Academy of Acute Care Physical Therapy, the American Thoracic Society, the CDC and WHO among other links embedded in this post. All the speakers have commented on the collaborative medical management and sharing of information in real time. It’s a gift to be able to listen to experts who speak and write well. Clinicians in the US are sharing information as rapidly as they get it from peers around the world in every area of healthcare, coordinating information within professions and between disciplines within hospital departments and among hospital systems and while working under extreme circumstances.
In healthcare there is known to be up to a 17 year lag in the translation of medical research into practice, not so with Covid-19. In an evolving pandemic, global sharing without the benefit of evidence-based support yet, has been the best way to function. Here are some things being said so far: According to the Seattle Intensivist US Covid 19 symptom presentations include:
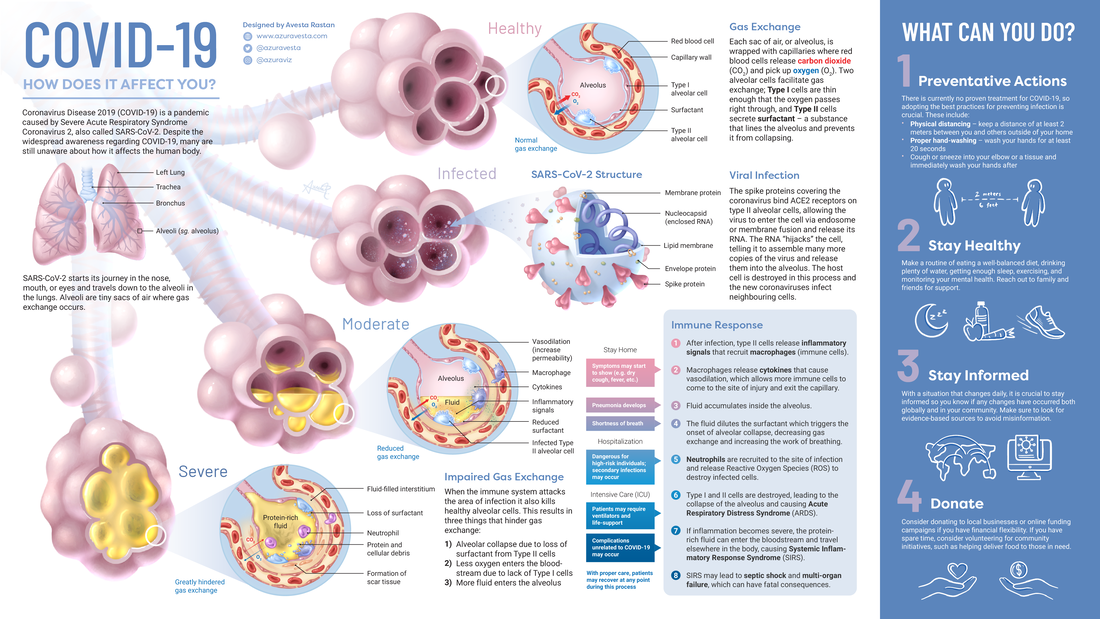
This is a different type of pneumonia than typical, unilateral pneumonia - it can be bilateral pneumonia in mild cases and progress to an Acute Respiratory Distress Syndrome which has the ability to affect multi organs. Systemic inflammation may be responsible for acute kidney, cardiac and neurologic events. The disease results in a perfusion mismatch between blood in capillaries and the flooded alveoli (shown in the brilliant image at the start of this post; source here). That failure to effectively oxygenate the alveolus results in increased work at rest to get oxygen to the body tissues, which multiplies with activity. Because the location of the inflammation (capillary) and alveolus are more peripheral and posterior in the lung, lying on belly has been advocated for those with the virus for facilitation of oxygenation. According to the American College of Cardiology the overall case fatality rate is 2.3% however fatality rates increase with age and with comorbidities specifically:
In just 1-2 weeks a very robust healthy person might look like an end stage lung transplant patient due to the speed of deterioration in the lung at the alveoli (gas exchange) level. Additionally, while typical pulmonary impaired patients have a more gradual deterioration to end stage and develop adaptive responses and awareness, the covid patient’s oxygen exchange destruction is much more rapid and makes them understandably highly anxious as a result of impaired oxygenation and resultant skeletal muscle weakness. The recovered patient will have significant muscle weakness and drastically poor endurance as a result of the sequela and the severe immobilization when acutely ill. I hate to be self promoting so let me promote all of the service providers at EngineHouse16 as being necessary to the recovery of these patients after hospital and subsequent home healthcare discharge. Skilled nursing and rehabilitation units will not be the environment these folks will be sent to. In addition to the preventive measures we already know, it might be wise to add or increase your present movement/activity level and include muscle strengthening. Because of the way the lung is impacted by pneumonia there may be benefit in learning while still healthy, how to do diaphragmatic breathing as shown here. Additionally, while there are videos about breathing techniques circulating on the internet there has long been fundamental advice for those who have difficulty breathing normally, to sleep with the head of the bed elevated or using extra pillows, and to sleep or lie in a variety of postures rather than solely on ones back. Lying on ones belly can have orthopedic contraindications so please be in touch with questions in that regard, it is not appropriate for everyone, and does not prevent illness. And defer to your pulmonologist for those with obstructive or restrictive lung conditions. I’ve included a differential chart here from the CDC and WHO not because it helps tease covid out from the flu, because it does not, but to highlight how similar the common cold and seasonal flu are. People often think of the flu as being a gastrointestinal issue perhaps with diarrhea when in fact it really may present identically to the common cold except for the presence of fever. Point is, the hand hygiene, the facial restrictions, the cough containment, and the realization that all of our surroundings have always been contaminated is the best takeaway and we should always have been doing this stuff. Life with covid-19 around us may not have to be life altering, just a different way of thinking about our surroundings. |
Author:
|
Perspectives for Patients:
 RSS Feed
RSS Feed
Proudly powered by Weebly